Voice Assessment for Individuals with ALS
Why assess voice?
A multi-faceted approach to assessment of voice in ALS is necessary to determine the ways in which the voice of an individual with ALS is affected by the disease and to provide data to make a decision about the best course of treatment. It is further important for SLPs to be able to identify signs of neurological disease within an assessment because voice can be one of the first symptoms of a disease. Specifically with ALS, it has been proven that dysphonia appears before dysarthria, so sensitive parameters to define laryngeal involvement are needed even before a client presents clinically with the disease (Robert et al., 1999). We need to make a correct and thorough diagnosis with any necessary referrals to help our clients receive the best care possible at the earliest time. Current evidence points to a combination of perceptual and instrumental methods in voice assessment of ALS (Bunton et. al, 1999 & Robert et al., 1999).
Checklist to assist in the diagnostic process:
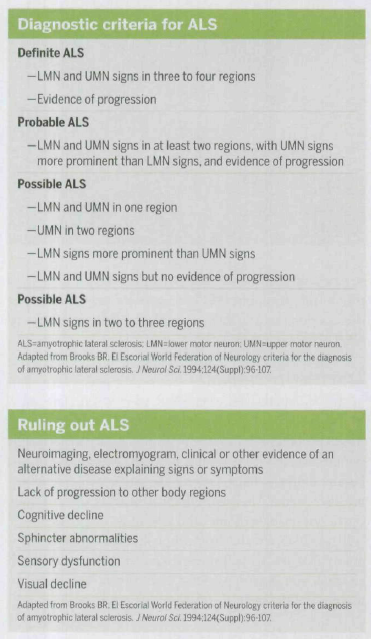
(Grief, 2008)
Perceptual Evaluation
The key voice characteristics observed in clients with ALS by using perceptual evaluations include lower than average pitch with slightly modulated intensity, hoarseness, strained voice, breathy voice, and vocal tremor (Robert et al., 1999). Other studies show hypernasality, imprecise articulation particularly related to insufficiency in velopharyngeal valving and lingual function, harsh vocal quality, audible inhalation, and slow or fast speaking rate (Turner & Weismer, 1993 & Kent et al., 1992). In regards to the timing of speech, individuals with ALS have been observed to have effortful, slow productions with short phrases, inappropriate pauses. Further characteristics include decreased pitch and loudness range, pitch abnormalities, glottal fry, and a slurred speech sound caused by muscle weakness (Watts & Vanryckeghem, 2001). Agreement on a set list of voice symptoms for ALS in literature is difficult because the dysphonia of ALS is masked by the dysarthria (Robert et al., 1999). This causes both symptoms and judgments about primary voice characteristics to vary widely.
Perceptual Evaluation Protocol
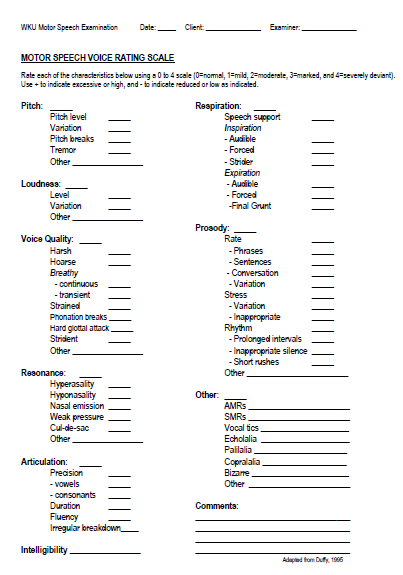
(SLP 508 - WKU)
Functional Rating Scale
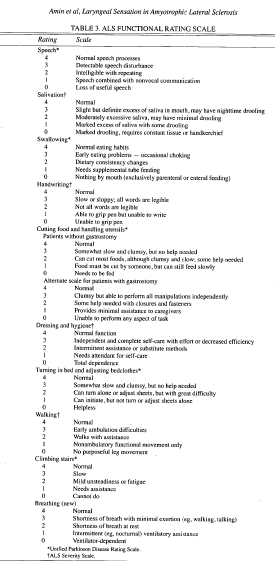
(Amin et al., 2006)
Instrumental Evaluation
A more data driven approach to assessment of voice disorders in clients with ALS involves the use of acoustic measures in instrumental evaluation. While the acoustic measures below provide the SLP with good, hard data, it is not a replacement for clinical observation and knowledge and should be used in conjunction with the perceptual evaluation. It is, however, beneficial to use an instrumental evaluation particularly with early identification because it has been reported that acoustic analyses can detect laryngeal abnormalities in patients with ALS before perceptual evaluations indicate voice dysfunction (Kent et al., 2003). Important data to gather in the study of voice disorders related to ALS include Fo (Hz), jitter (%), coefficient of variation for frequency (%), intensity (dB), shimmer (%), coefficient of variation for intensity (%), number of harmonics, and frequency range (Hz) (Robert et al., 1999). An examination of data from clients with ALS overall show an increase in jitter and shimmer (parameters measuring aperiodicity of frequency and intensity, respectively) and a decrease in the noise-to-harmonics ratio (a parameter measuring the turbulent noise occurring when full glottal closure is not achieved during phonation) (Robert et al., 1999). Additional findings show decrease in frequency range, a reduction in the mean slope of the second formant (F2) when performing a spectral analysis, and abnormal fundamental frequency values (either higher or lower than normal) (Kent et al., 1992). These differences occur as a result of the same disease because corticobulbar involvement may dominate, which causes hyper-adduction of the vocal folds, or bulbar involvement may dominate, which causes hypo-adduction of the vocal folds (Watts & Vanryckeghem, 2001). Furthermore, a reduction in frequency range can be apparent in clients with ALS even before any other notable changes occur in their voice (Robert et al., 1999). Data from an instrumental evaluation may be the first sign that a client has ALS.
Specific instruments used in the literature for acoustic analysis of voice disorders in clients with ALS include the EVA objective voice analysis system (CNRS, Marseille, France), the Kay 5500 Digital Sonagraph (Turner & Weismer, 1993), the Kay 7800 Digital Sonagraph (Kent et al., 1992), Cspeech (Bunton et al., 1999), the demodulator (Winholtz & Ramig, 1992), the Multi-Dimensional Voice Program (Kent et al., 2003), and the modulogram (Buder & Strand, 2003).
Specific instruments used in the literature for acoustic analysis of voice disorders in clients with ALS include the EVA objective voice analysis system (CNRS, Marseille, France), the Kay 5500 Digital Sonagraph (Turner & Weismer, 1993), the Kay 7800 Digital Sonagraph (Kent et al., 1992), Cspeech (Bunton et al., 1999), the demodulator (Winholtz & Ramig, 1992), the Multi-Dimensional Voice Program (Kent et al., 2003), and the modulogram (Buder & Strand, 2003).
Instrumental Evaluation Protocol
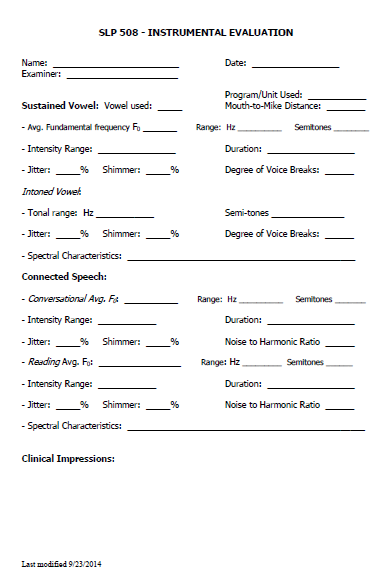
(SLP 508 - WKU)
Differences in instrumental evaluation results in an individual with no disease, an individual with pseudo-bulbar symptoms, and an individual with marked bulbar symptoms:



(Robert et al., 1999)
Modulogram
The modulogram is used to quantify and graphically represent long term modulations in the voice. The parameter and frequency domain of modulations are able to distinguish the phonations of persons with (ALS) from those of persons with multiple sclerosis (MS). The modulogram specifically analyzes modulations occurring in fundamental frequency and sound pressure level of the voice. Tremor, flutter, and wow are also analyzed. With an accurate voice diagnosis, better detection and differentiation of underlying diseases is possible, which leads to more precisely formulated clinical hypotheses and can best help the client.


(Buder & Strand, 2003)
Multi-Dimensional Voice Program (MDVP)
The Multi-Dimensional Voice Program (MDVP) has undergone clinical research and has been proven to be an effective assessment tool of voice disorders, particularly those caused by diseases such as ALS. The MDVP has the specific intent of being used for the characterization of a voice disorder and determining the specific cause of the voice disorder, for example discriminating between voice disorders caused by ALS or Parkinson’s Disease. The advantages of MDVP include the rapid, nearly automatic, measurement of multiple acoustic parameters for a selected voice sample. Some acoustic measurement devices can only analyze data from a sustained vowel phonation, but the MDVP is able to analyze data from connected speech. This is important because some voice dysfunctions only arise, or become more noticeable, in tasks such as connected speech (conversation, sentence repetition, or passage reading).


(Kent et al., 2003)
Oral Mechanism Exam

(http://speech-language-pathology-audiology.advanceweb.com/Features/Articles/Dysphagia.aspx)
A traditional oral mechanism exam should be included as part of the over-all assessment of voice disorders, particularly for clients with ALS. Key factors to look for related to ALS include reductions in tongue strength and velophrayngeal inadequacy (Kent et al., 1992). Other effects of the disease may also be noted at this time, particularly related to swallowing.
Laryngeal Exam
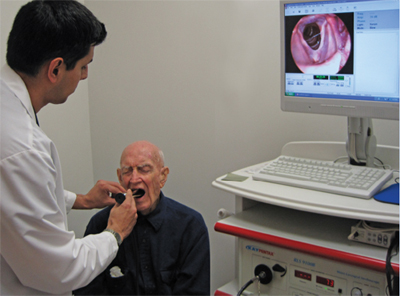
(http://www.holyname.org/md360/MarAprMay10/pa1.asp)
A laryngeal exam is necessary to view the function of the vocal folds and examine how their movement is affected by ALS. A flexible or rigid scope has been proven effective (Watts & Vanryckeghem, 2001). Hyper- or hypo- adduction of the vocal folds may be observed. A strained voice quality may be caused by increased spasticity of the folds (Robert et al., 1999). It is also important to complete a laryngeal exam in individuals with suspected ALS or similar disorders because research shows that clients who are not yet presenting with bulbar symptoms may still have laryngeal involvement (Robert et al., 1999). This will help in early detection and treatment.
Pulmonary Exam

(http://www.webmd.com/lung/ss/slideshow-bronchitis-overview)
Clients with ALS generally present with respiratory muscle weakness, which causes a reduction in the volume of expired air. Phonatory airflow may be further reduced by the hyper-adduction of the vocal folds. Aerodynamic parameters to focus on for clients with ALS include phonatory airflow (cc/s), cycle-to-cycle variation for phonatory airflow (%), and the coefficient of variation for phonatory airflow (%) (Robert et al., 1999). Other recommended data include measures of vital capacity, expiratory force, inspiratory force, and peak expiratory flow rate (Kent et al., 1992).
Ongoing Assessment
The above measures are useful not only for the initial assessment, but throughout therapy to track progress and guide the course of therapy. By performing ongoing assessments and sharing the data with clients along the way, clients will have a better understanding of the effects of disease progress on the laryngeal mechanism and the way therapy techniques are minimizing or modifying these effects (Buder & Strand, 2003 & Kent et al., 1992).
Page by: Kristina McIntyre
Main article used: (Robert et al., 1999)
Main article used: (Robert et al., 1999)
